The Relationship between Diabetes Mellitus and Periodontitis
Description
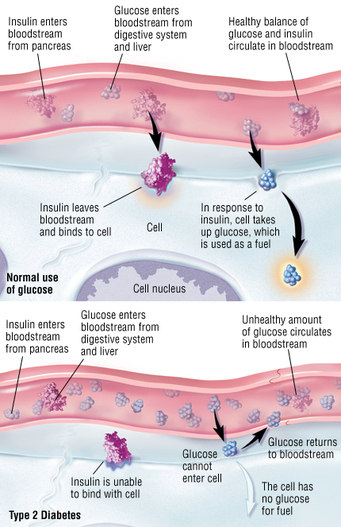
Diabetes is a disease where the body does not produce or properly use insulin. The body needs insulin to convert sugar, starches, and other types of foods into energy for the body to use in order to maintain life.
There are two types of diabetes: Type 1 and Type 2. Type 1 is termed insulin-dependent or juvenile-onset. With this type of diabetes, the insulin producing cells are damaged and cannot successfully produce its product resulting in high levels of glucose in the blood stream. Type 2 is termed non-insulin-dependent or adult-onset. With this type of diabetes, the body does not make enough insulin hormone and/or the cells of the body fail to use insulin in order to bring sugar into the cells.
Patients with diabetes are of concern for the dental practice due to the increased risk for periodontitis. Patients with well controlled diabetes and good oral hygiene are not at an increased risk for periodontitis, however, if they have uncontrolled diabetes, their risk significantly increases. Even more so if they smoke.
Diagnostic Factors
Diabetes may be present for a long amount of time before it is successfully diagnosed. For this reason, dentist may be the first health care provider to detect diabetes. Gingival and periodontal signs that the clinician should be aware of:
Etiology
Type 1: destruction of insulin-producing cells of the pancreas
Type 2: insufficient production of insulin and/or cells of the body fail to use insulin
Excess amounts of sugar can alter the phenotype of macrophages and other cells responsible for removal of pathogens from the tissues, stimulation of inflammatory response, metabolism of fibroblasts and lymphocytes and stimulate bone resorption by prostaglandins. Macrophages are the key cells in the pathogenesis of periodontitis through the production of cytokines. This negative phenotype-altering reaction potentially causes the macrophage to become destructive producing uncontrolled pro-inflammatory cytokines. Also, there is a reduction in neutrophils which function as a primary defense for the periodontium. This decrease is observed in patients with diabetes and is considered another mechanism that increases periodontitis susceptibility.
Associated Pathogens
The pathogens associated with periodontitis and its link with diabetes are the periodontitis pathogens A. actinomycetemcomitans, P. gingivalis, T. forsythia
AAP Classification System
IV-C: Periodontitis as a Manifestation of Systemic Diseases not otherwise specified
Prevalence
Type 1 diabetes accounts for approximately 10% of all diagnosed diabetes cases.
Type 2 diabetes is the most common form usually occurring after the age of 40.
-Diabetes in patients with periodontitis is greater by two times than in people without periodontitis
-Increasing number of cases seen in Indian communities
Patient Education
The patients should be educated on the side effects diabetes can have on their oral health. They should also be aware of the importance of high standard at home daily oral hygiene. This includes bushing, flossing, interdental brushes, and in some cases require the use of chlorhexidine mouthwash or gel twice per day. The patient also needs to have frequent professional care visits to help maintain oral health. The patient should be instructed to be sure to take the proper medications to keep their diabetes controlled and also, should practice a healthy eating and exercise regimen.
Treatment Recommendations
Diabetic patients should be seen in the morning and appointments should be short in length. When confirming appointments be sure to instruct the patient to eat before their appointment and obtain their numbers the evening before or the morning of the appointment.
Maintenance Recommendations
>great at home oral hygiene
>frequent professional care visits in 3-4 month intervals
>maintain contact between physician and dentist
>keep diabetes controlled
Reference
Hussain, A. M. (2011). The Relationship between Diabetes Mellitus and Periodontitis. Al Ameen Journal Of Medical Sciences, 4(1), 84-86.
Ibsen, O. Andersen Phelan, J. Oral Pathology for the Dental Hygienist, Fifth Edition.
Nield-Gehrig, J., Willmann, D., (2011). Foundations of Periodontics for the Dental Hygienist, Third Edition
Additional Information
Photos from Google images
Article from Ebscohost
Diabetes is a disease where the body does not produce or properly use insulin. The body needs insulin to convert sugar, starches, and other types of foods into energy for the body to use in order to maintain life.
There are two types of diabetes: Type 1 and Type 2. Type 1 is termed insulin-dependent or juvenile-onset. With this type of diabetes, the insulin producing cells are damaged and cannot successfully produce its product resulting in high levels of glucose in the blood stream. Type 2 is termed non-insulin-dependent or adult-onset. With this type of diabetes, the body does not make enough insulin hormone and/or the cells of the body fail to use insulin in order to bring sugar into the cells.
Patients with diabetes are of concern for the dental practice due to the increased risk for periodontitis. Patients with well controlled diabetes and good oral hygiene are not at an increased risk for periodontitis, however, if they have uncontrolled diabetes, their risk significantly increases. Even more so if they smoke.
Diagnostic Factors
Diabetes may be present for a long amount of time before it is successfully diagnosed. For this reason, dentist may be the first health care provider to detect diabetes. Gingival and periodontal signs that the clinician should be aware of:
- persistent gingival inflammation after phase-I nonsurgical periodontal treatment (supra/sub gingival scaling and cleaning, oral hygiene instruction)
- severe gingival inflammation response to plaque and alveolar bone loss despite periodontal treatment
- severe, aggressive periodontitis in patients 20-45 years old (deep periodontal pocketing, increase tooth mobility and tooth migration, causing teeth to over erupt or spaces to open between teeth, and radiographic evidence of advanced bone loss)
- continual formation of periodontal abscesses
Etiology
Type 1: destruction of insulin-producing cells of the pancreas
Type 2: insufficient production of insulin and/or cells of the body fail to use insulin
Excess amounts of sugar can alter the phenotype of macrophages and other cells responsible for removal of pathogens from the tissues, stimulation of inflammatory response, metabolism of fibroblasts and lymphocytes and stimulate bone resorption by prostaglandins. Macrophages are the key cells in the pathogenesis of periodontitis through the production of cytokines. This negative phenotype-altering reaction potentially causes the macrophage to become destructive producing uncontrolled pro-inflammatory cytokines. Also, there is a reduction in neutrophils which function as a primary defense for the periodontium. This decrease is observed in patients with diabetes and is considered another mechanism that increases periodontitis susceptibility.
Associated Pathogens
The pathogens associated with periodontitis and its link with diabetes are the periodontitis pathogens A. actinomycetemcomitans, P. gingivalis, T. forsythia
AAP Classification System
IV-C: Periodontitis as a Manifestation of Systemic Diseases not otherwise specified
Prevalence
Type 1 diabetes accounts for approximately 10% of all diagnosed diabetes cases.
Type 2 diabetes is the most common form usually occurring after the age of 40.
-Diabetes in patients with periodontitis is greater by two times than in people without periodontitis
-Increasing number of cases seen in Indian communities
Patient Education
The patients should be educated on the side effects diabetes can have on their oral health. They should also be aware of the importance of high standard at home daily oral hygiene. This includes bushing, flossing, interdental brushes, and in some cases require the use of chlorhexidine mouthwash or gel twice per day. The patient also needs to have frequent professional care visits to help maintain oral health. The patient should be instructed to be sure to take the proper medications to keep their diabetes controlled and also, should practice a healthy eating and exercise regimen.
Treatment Recommendations
Diabetic patients should be seen in the morning and appointments should be short in length. When confirming appointments be sure to instruct the patient to eat before their appointment and obtain their numbers the evening before or the morning of the appointment.
Maintenance Recommendations
>great at home oral hygiene
>frequent professional care visits in 3-4 month intervals
>maintain contact between physician and dentist
>keep diabetes controlled
Reference
Hussain, A. M. (2011). The Relationship between Diabetes Mellitus and Periodontitis. Al Ameen Journal Of Medical Sciences, 4(1), 84-86.
Ibsen, O. Andersen Phelan, J. Oral Pathology for the Dental Hygienist, Fifth Edition.
Nield-Gehrig, J., Willmann, D., (2011). Foundations of Periodontics for the Dental Hygienist, Third Edition
Additional Information
Photos from Google images
Article from Ebscohost
